Semaglutide, tirzepatide, and the broader class of GLP-1 receptor agonists have changed the weight loss landscape. The clinical results are undeniable: participants in the STEP trials lost an average of 15 to 17% of their body weight over 68 weeks. But buried in that headline number is a problem that most prescribing physicians are not discussing with their patients.
Not all of that weight loss is fat.
The Muscle Loss Problem
A 2022 analysis published in Diabetes, Obesity and Metabolism found that approximately 25 to 40% of weight lost on GLP-1 medications comes from lean mass, which includes muscle tissue. In practical terms, if you lose 40 pounds on semaglutide, 10 to 16 of those pounds may be muscle, not fat.
This matters enormously for long-term health. Skeletal muscle is not just about strength or appearance. It functions as a metabolic organ, regulating glucose disposal, insulin sensitivity, and resting metabolic rate. Losing significant muscle mass while on a GLP-1 drug can lower your basal metabolic rate, making it harder to maintain weight loss after discontinuing the medication. It can also accelerate age-related sarcopenia, the progressive muscle loss that begins in your mid-30s and accelerates after 60.
Peter Attia, M.D., has been vocal about this concern: the scale going down is not inherently good if the composition of that weight loss is working against your long-term metabolic health.
Why a Scale Is Not Enough
A bathroom scale tells you one number. It cannot distinguish between fat mass, lean mass, bone mineral content, and water. Two people can lose 30 pounds and have dramatically different outcomes. One may have preserved muscle and lost primarily visceral and subcutaneous fat. The other may have lost substantial muscle along with fat, leaving them lighter but metabolically worse off.
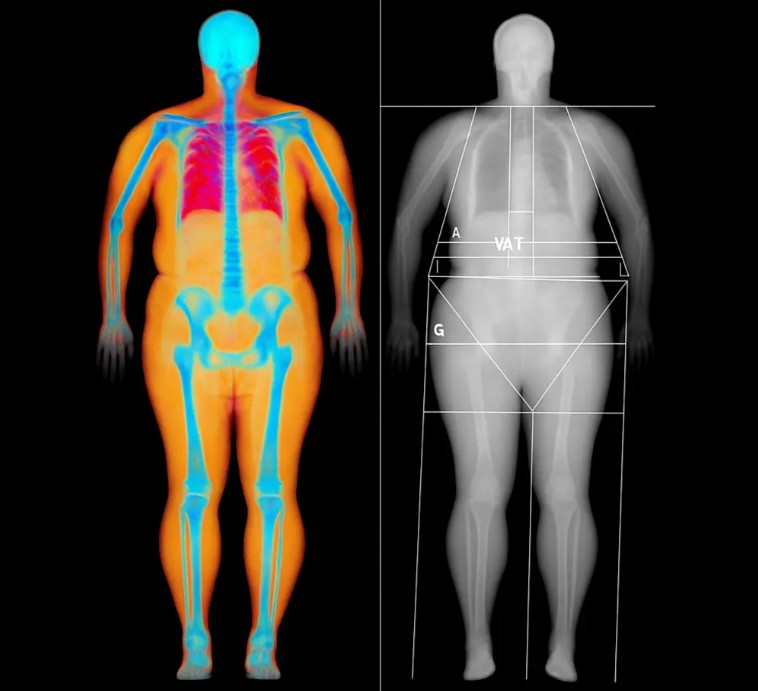
This is where DEXA scanning becomes essential. A DEXA scan provides a precise breakdown of your body composition across all three compartments: fat mass, lean mass, and bone mineral density. It shows you exactly what changed, how much, and where. For someone on a GLP-1 medication, this is not optional information. It is the difference between informed treatment and flying blind.
The Intervention Window
The good news is that muscle loss during GLP-1 therapy is not inevitable. It is manageable with the right interventions, but only if you know it is happening. Research from the New England Journal of Medicine has shown that combining semaglutide with structured resistance training significantly reduces lean mass loss compared to medication alone.
The two primary levers are resistance training and protein intake.
**Resistance training** sends a strong anabolic signal to muscle tissue, essentially telling the body “this muscle is being used, do not break it down for energy.” Three to four sessions per week of progressive resistance training, focused on major compound movements, is the current evidence-based recommendation for patients on GLP-1 drugs.
**Protein intake** is the raw material for muscle protein synthesis. Most clinical guidelines for GLP-1 patients suggest 1.2 to 1.6 grams of protein per kilogram of body weight daily. However, some researchers argue that patients actively losing weight should target the higher end of that range, or even 2.0 g/kg, to maximize muscle preservation.
What a Monitoring Protocol Looks Like
A responsible GLP-1 monitoring protocol using DEXA should include a baseline scan before starting the medication (or as soon as possible after starting), a follow-up scan at 3 to 4 months to assess the ratio of fat loss to lean mass loss, and subsequent scans every 4 to 6 months for the duration of treatment.
At each scan, you are looking at total fat mass change, total lean mass change, regional lean mass (arms, legs, trunk) to catch asymmetric muscle loss, visceral adipose tissue (VAT) to confirm you are losing the most dangerous fat first, and bone mineral density to flag any bone health concerns early.
If a scan reveals that lean mass is dropping faster than expected (more than 30% of total weight loss), the protocol shifts: training volume and intensity increase, protein intake is optimized, and in some cases the GLP-1 dose is adjusted in consultation with the prescribing provider.
Why This Matters at Plus10
At Plus10, we see this intersection of pharmacology and physiology as one of the most important conversations in health right now. Our on-site Nurse Practitioner works directly with members on GLP-1 programs, providing clinical oversight, prescriptions where appropriate, and coordinated care that connects the medication to the data.
A DEXA scan is the objective check on whether your treatment is doing what you want it to do. Without it, you are relying on a scale and a mirror, and neither one tells you what is happening to your muscle mass, your bone density, or your visceral fat.
The combination of GLP-1 therapy with structured DEXA monitoring, progressive resistance training, and targeted nutrition is not a trend. It is the evidence-based approach to making sure the weight you lose is the right kind of weight.
[Explore testing and membership options](https://plus10life.com/our-pricing-2/)
**Contact:** info@plus10life.com | 400 Gerault Rd, Flower Mound, TX 75028